 “I was always very active, ate well, etc. I never thought I'd experience challenges and setbacks regarding my health. However, in 2013, I had my first, major intracerebral hemorrhage. It was caused by a CVA (cavernous amgioma) or CVM (cavernous malformation). A CVA is a cluster of blood vessels that leak through their own walls. Mine was located deep within my brain, in an area my neurosurgeon called "high real estate". Surgery was too risky. We hoped that this would be a one time event. Unfortunately, I had several more bleeds and another major hemorrhage in 2016. To save my life, they had to operate. I am extremely fortunate to be alive despite my cognitive and physical deficits. I'm in pain continually. But nature is my therapy, and I get out as much as I can. My advice? Accept help. Much love to all misfit hikers out there!—Dana, (@mrs.hangle).
. Pronouns: She/Her . Dana would like to give a shout-out: I am not affiliated with a group, but one thing I feel strongly about is the appropriation of Indigenous traditions and ceremonies in ecotherapy. I would just encourage people to refrain from partaking in cultural activities, which are not their own. Don't be taken financially and emotionally by people claiming to be able to use Indigenous events in nature if they are not Indigenous themselves. In kindness, Dana
1 Comment
 How do you medically advocate for yourself? For those of you that follow along, you know that I went to the Cleveland Clinic main campus ER about a month ago for a severe back pain issue and the experience was less than stellar. It was actually awful, mainly because the doctor failed to adequately manage the pain, attempt to find a diagnosis, or come up with a treatment plan. I did a follow up post regarding the very well documented dismissal of women, people of color, people of size, etc. who complain of pain. So now, the final post - how to medically advocate for yourself.
It's important to be able to do so, especially if you're an adventurer, because even if you don't have chronic pain there's a fairly high likelihood that you'll injure yourself in some way at some point. So here's a few tips and tricks to make sure that you're diagnosed and treated. Do not let them shame you. Being fat or old or gay is not a moral issue. YOU ARE A PERSON AND DESERVING OF TREATMENT. Do not allow yourself to be dismissed - you know your body - insist on care. It could save your (or a loved one's) life. If you're doctor isn't taking your pain or issue seriously, ask for another doctor. You're having real fucking symptoms, don't let them make you feel bad for having them. When my grandmother had a stroke, she was definitely not getting the care she needed at the rinky dink hospital she was at. They refused to do any tests to see if she'd had a stroke, etc. In fact, they insisted she was simply dehydrated and refused to do anything at all except IV saline. We insisted she be transferred to another hospital, which took my father and I driving to main and not budging an inch. The doctor was later fired, and my grandmother was transferred to a larger hospital able to get her the care she needed (and responded to). If you have a chronic issue or long-term disease, carry your medical records with you. You can get a free dropbox account to store them, or email them to yourself. Don't depend on your phone, in case you don't have it when you go. Next, question, question, question and be sure to communicate concerns and desires. There are some questions you can write out beforehand (and give to a friend), so they're stuck in your mind and ready to go. When in the ER, especially, it can be stressful and overwhelming, making it very easy to get confused/forget to ask the important stuff. Some questions to ask if you go to your regular doc/doc in a box: - What do you believe the issue is? - Why do you believe it is xyz? - Is there a test to confirm that? Why are you/are you not confirming? - I am in a significant amount of pain - what is the plan to treat it? Why are we treating it in that way? - Why hasn't my pain been addressed yet? - If your symptoms persist, do NOT be afraid to go to another doctor, even if you like the one you have. Different doctors have different knowledge bases and experiences. If you’re in the Hospital or ER, then add these questions on:
I'd like to mention that the Cleveland Clinic is one of the top rated hospitals in the country. I have had wonderful treatment there. However, this ER needs to get its shit together. I still have nightmares about it. I'm definitely implementing these, so I can be better prepared if there's a next time. Hopefully, they also help you or a loved one. If you have any tips to add, please feel free to comment below or contact me here.  The pain is just in your head...that's how I felt when I went to the Cleveland Clinic downtown ER just over a week ago. The doc implied I was in pain because I was fat, had over-exercised, or that I was simply drug seeking. It was such an awful experience that I wanted to see if I was the only one. I felt very much alone and I started to doubt myself which I rarely do. Then I started reading. And holy shit. Sorry not sorry for the length of the post. It's important shit, and if it's 400 words over what people will typically read, well, if you can make it through a Stephen King novel, you can hopefully hang on long enough to make it through here.....
This isn't made up - it's a valid problem, as reported on by the NY Times, Harvard Health, and the Washington Post. So what's happening? Well, unfortunately, if you aren't a white cis male and in pain, good luck:
Why? Why does this happen? You can't ignore that white cis men have certain societal privileges, leftover from a thousand years of being the top dogs. I have nothing against white cis males - my problem is with the people that afford them the privilege at the expense of others. There's a historical connection that can't be ignored - for example, studies have shown in the case of women, doctors are much more likely to assume women’s pain is caused by emotional issues and/or hysterics rather than rooted in actual physical causes. EVEN WHEN CLINICAL TESTS CLEARLY DEMONSTRATE THEIR PAIN IS REAL AND IDENTIFIABLE. Not only that, but women with emergent or chronic pain are much more likely to be misdiagnosed as having a mental health issue and prescribed anti-anxiety or psychotropic drugs. I guess that's progress from the forced masturbation doctor's prescribed in the 1800s. Additionally, lady folk with biologically female issues in the ER and out of the ER, who complain of pain associated with fibroids or endometriosis are still often dismissed in high numbers as having pain “normal to being a woman.” It boils down to doctors believing women are more emotional and irrational than men, and so over exaggerate their pain, if they are actually having pain at all. This isn't anecdotal - Karen Calderone, for example, found doctors tend to treat men and women differently when they’re in pain, even when they exhibit the same symptoms. And they’re given sedatives instead of pain-managing drugs. Because the pain is in their head and will go away if they get their hysterical vaginas under control. WTAF. The internalized discrimination is immense in the medical community. In 2016 nearly 50% of those medical students and residents surveyed believed at least one myth regarding race and pain – like believing black people had nerve endings that are less sensitive than whites. Uh, what? Like, what the what? Doctor’s also erroneously believe that women and persons of color are more likely to become addicted to painkillers, because they’re more likely to abuse them. And these are only a few examples. If you’re attractive? Ha. Good luck to you. The ER is one place that shit will work against you. Why? Because is you’re pretty on the outside, it means you’re healthier on the inside and therefore you’re less likely to be treated for serious health issues. Yikers. Basically, unless you’re a white, heterosexual male, you’re kinda fucked. Older? Told the pain is part of aging and to suck it up. LGBTQ? Hysterical. Children? Whiney. The list goes on. So what kind of ramifications does this have? The answer is….a lot. Medical research on women lags behind, and it's killing us - A study published in 2000 by The New England Journal of Medicine found that women were SEVEN TIMES more likely to be discharged from an ER in the MIDST OF HAVING A HEART ATTACK. Why? Because all the studies on heart attack symptoms are done on men and women have different symptoms. What about abdominal pain? Head pain? Back pain? Pain is an indication that something is wrong. Get the pain under control and then figure that shit out. Don’t send us home. Don’t ignore us. Don’t patronize us. When you do, we live in pain and illness much longer than necessary. Sometimes, it's never treated. Women and persons of color are also less likely to seek medical attention, out of fear of being dismissed or ignored. So the problem worsens. Or we just die. I run a group for misfits - those that don't fit the stereotype of the "typical" outdoor person. Outdoors adventures. Sometimes we're going to get hurt. Sometimes we're going to have chronic problems and/or pain. We also deserve to be cared for, to be treated in a fair and equitable way. When you don't, you further limit our access. Stop it. I posted what happened and I've now looked in to why it happened. Next up, what can be done? It's not enough to complain, I want to find solutions. What do YOU think people can do? What the solution is? Post below or contact me here. 
Lucy ponders the correct direction.
I don't like to hike in fear, but I do like to hike in safety. Why get a satellite communicator? Cause they're fucking awesome. And not just for hiking - they're great for anytime who might be in a remote area and not have cell service. I couldn't find the article (of course), but I'd read something like 60% of SOS calls from satellite locators are by people that have been in a car accident. Legit. They aren't just for hikers, but joggers, walkers, anyone that's gonna be outdoors....
Sample Uses:
What They Offer: Varies drastically depending on the model.
Biggest Downside - Price. They're a chunk of cash, ranging from $150.00 up to $1200.00 and beyond. On top of that, you have to get a subscription. The plans range in price, depending on what features you want - I have one that costs $11.00 a month. I'm big on access - and safety - for everyone. And these are prohibitively expensive for many, even with sales. I don't like the idea that because people can afford this, they're safer on the trails. Other Downsides: They don't really work in caves and inside homes. They can also get a bit sketch if the sky is occluded (heavy tree coverage, etc.), but most models have a means to continually attempt to send the message until it gets through. If you're thinking about getting one (they're hella on sale with the holiday), check out this article from REI on selecting the best one. Over the next week or so, I'll be reviewing the Spotgen 3 and the Garmind InReach Mini. One is amazing and one is....not. Do you have a satellite communicator? Love it? Hate it? Ever had to use it? Comment below or email me here! 
No More NSAIDs for me!
"Lots and lots of Vitamin I," a guy replied (laughing) to me the other day, while we were chatting at the physical therapist's office, after I'd queried how he kept up his really intense workout regime with the type of injury he had.
Inwardly, I cringed. Bigly. What's Vitamin I? It's what outdoor folks (particularly thru hikers and hikers) fondly call Ibuprofen, an NSAID, and it's no joke. What's an NSAID? It's a lovely anti-inflammatory drug you can buy over the counter at any pharmacy - it's great for pain and marvelous for inflammation. It's not a steroid and you can buy it everywhere, so it's safe, right? Wrong. When my back injury occurred, the docs started me on large doses of Vitamin I, which I was on for weeks - which totally destroyed my stomach. As in I can't eat the same way I used to, I have a lot of pain with it, and I have had to change how I do things because of it. It's greatly affected my everyday life. There's been a lot of studies, and you can read an overview of them at Time, the Cleveland Clinic, the Mayo Clinic, and Harvard's websites. So what are the risks of NSAIDS? - The heart - increased risk for heart attack by 1/3 (though Ibuprofen more than doubled those risks).....and 19% increased risk of being hospitalized for heart failure - intestinal bleeding - increase chance of stroke - increase change of hearing loss (by 10%) - greater chance of bone loss with resistance training But you only take them occasionally in low doses, so that's fine, right? Nope. You can mess your heart up only using it for less than a week - though long-term use and higher doses increase the risk. Even scarier - they don't know why it increases the risk of a heart event. WTAF. Sometimes, you may *have* to take it, to get some sleep, especially if you manage chronic pain. Don't feel bad about it!! - take the lowest dose possible - don't take more than one kind of NSAID at a time, it increases the danger What if you have chronic, painful inflammation and don't want to take "Vitamin I" any longer? Look for my post next week, where I'll write about some of the wonderful alternatives out there to help deal with inflammation. Because being in pain sucks, and it keeps you from doing the &^%$ you want to do. Do you use NSAIDS? Any problems? How do you deal with pain from activities? Comment below or email me here.  I'm sure many of you have seen the viral video of Amy Cooper calling the police on Christian Cooper, an African American bird-watcher who was enjoying the Bramble in New York earlier this week. She called the police because he asked her to put her dog on a leash (park rules). She says in the video, "I'm going to tell them there's an African American man threatening my life." She tried to use this man's race as a weapon against him. The outdoors is political, don't let anyone ever tell you otherwise. When I first googled top 25 hiking blogs of 2019, I was really surprised. The first several sites that listed blogs included very few women and I didn’t visually identify (or see in the descriptions) any minorities. Or people with disabilities. Or Pride Pack members. Or fat people. Everyone looked very, very white. I taught Diversity in America for quite a few years at several local colleges. I don't know why I was surprised at the lack of diversity in the online presence for outdoor adventures in the U.S., since there's a definitive lack of representation on trails. When my friend told some co-workers he was going backpacking for the weekend, his African-American buddy responded along the lines of, “Only in America would white people go in to the woods and pretend to be homeless.” It bothered me on a level that was difficult for me to define, because I view the outdoors as such an important part of who I am. It's a privilege. And privilege and access is a big part of the problem - because it isn't that way for everyone. The Outdoor Foundation, who conducted a survey in 2013, found that 73% of participants in outdoor activities were white, and 47% had an income above $75K (You can read the entire report on their website here.). 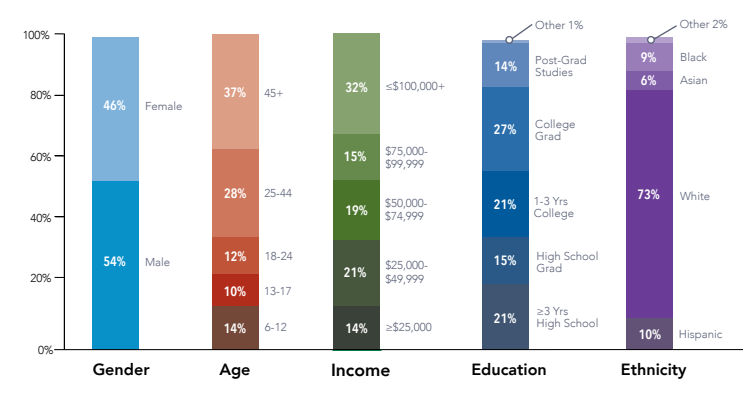 And when whites in the U.S., on average, are the ones making that higher income, it's indicative of a problem and not just in relation to getting folks in to the great outdoors. 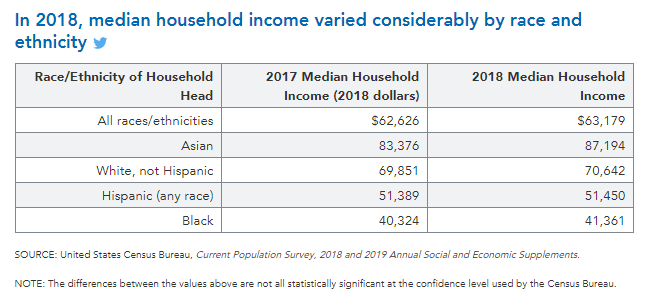 Who's involved matters, too - from how outdoor events and activities are marketed to who runs the parks programs, you'll see primarily white people. The Green 2.0 Report demonstrates a clear lack of diversity in the government agencies, foundations, and NGOs that oversee outdoors recreation and upkeep: 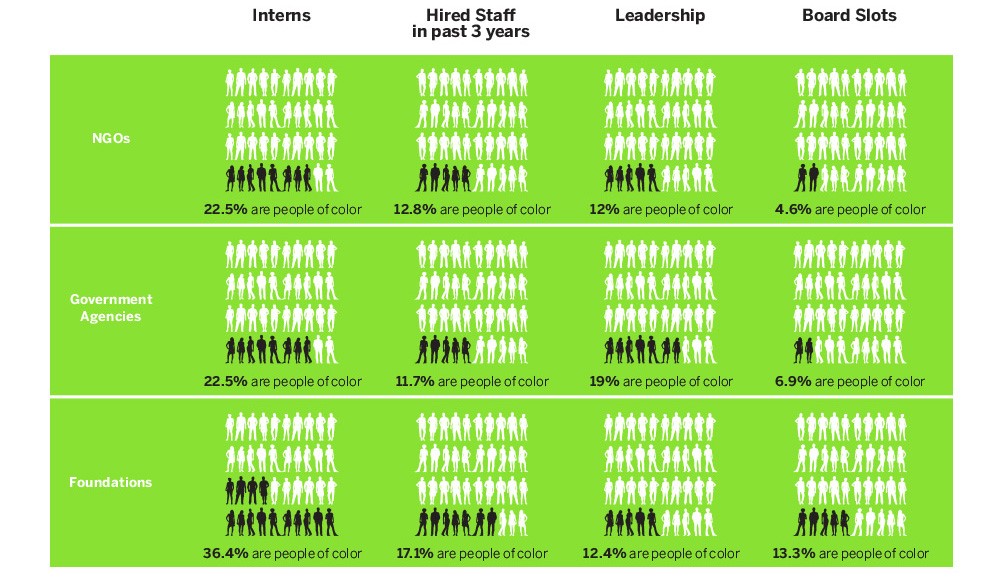 The world is a changing place, and it’s time for more outdoor activities, and the folks that are already involved in those activities, to change with it.
Race and ethnic minorities made up 40% of the U.S. population in 2016, and those numbers continue to increase. Consider the words of Teresa Baker, a contributor for The Bold Italic, when she wrote “The climate is changing, and so are the demographics of our country. What will happen when, in two to three decades, our new, non-white majority in the US doesn’t care about the environment due to a lack of involvement now?” While I fit the definition of a Misfit Hiker & Adventurer for a number of reasons, I am, in fact, white. So I come at this, clearly, from a very different perspective. I'd like to note that I am not here to define for anyone else what experiences they should have in the outdoor world or how they should feel about those experiences and/or interactions. However, what I can do, is try to make those outdoor spaces more welcoming. I can conduct and relate research in to different issues. And I can showcase others opinions, viewpoints, and experiences. Misfit Hikers is about inclusion and representation, and you're going to find a lot of emphasis on how people access (or don't access) the outside world of adventuring. And what actions can be taken to address identified issues. As a former teacher, I'm a big fan of education and considering other viewpoints - it forges a connection and helps shape how we view the world (and others). My very small first action is to start gathering resources on different topics regarding inclusion and representation in the outdoors. You can find the start of my efforts here. If you know of an article, website, Instagram, etc. that you'd like to see included, please comment! Or feel free to email me. What happened to Christian Cooper shouldn't ever happen. As stewards of the outdoors we need to - have to - do better. |

Archives
March 2021
Categories
All
|